

On Patient Safety & Shame
Enlightened Centrism Strikes Again
Let's review the facts for a moment:
Over a million Americans have been killed by the SARS-CoV-2 virus.
Many more millions of Americans have wound up with crippling disabilities, long-term health complications, and other issues as a result of infection with the SARS-CoV-2 virus, commonly referred to as “Long COVID.”

In a battlefield scenario, we wouldn't discriminate between a soldier who dies instantly from a 7.62mm bullet to the skull, and the one who has his arm blown off by an Improvised Explosive Device (IED) but survives. They are both considered “casualties” that weaken the overall effectiveness of the cohesive unit.
Total national casualties of the SARS-CoV-2 pandemic are currently around 20-25 million. Nearly every single one of these casualties were infected by their fellow American citizen. More importantly, countless chains of viral transmission were forged that inevitably ended in somebody dying - or winding up horribly disabled.
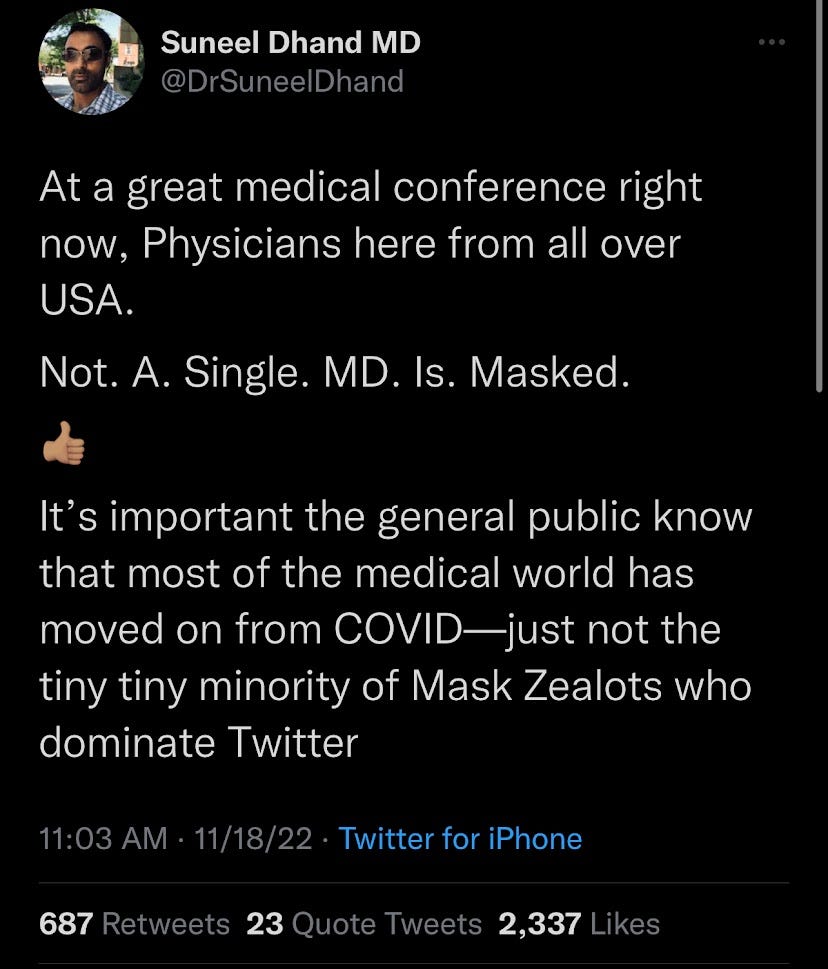
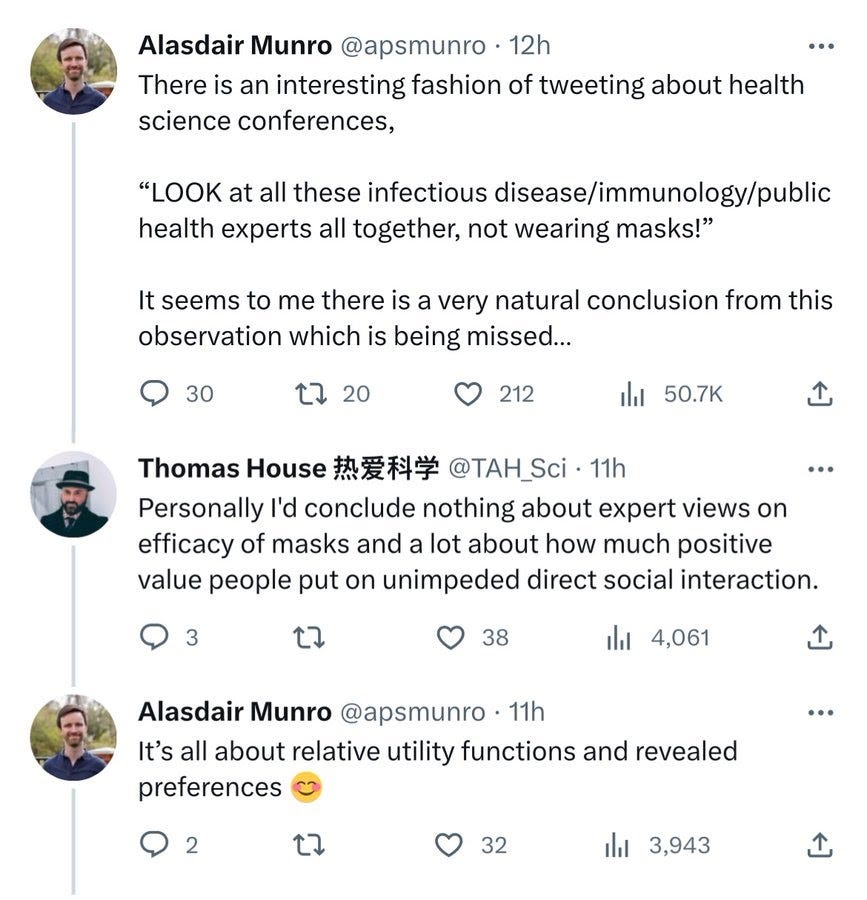
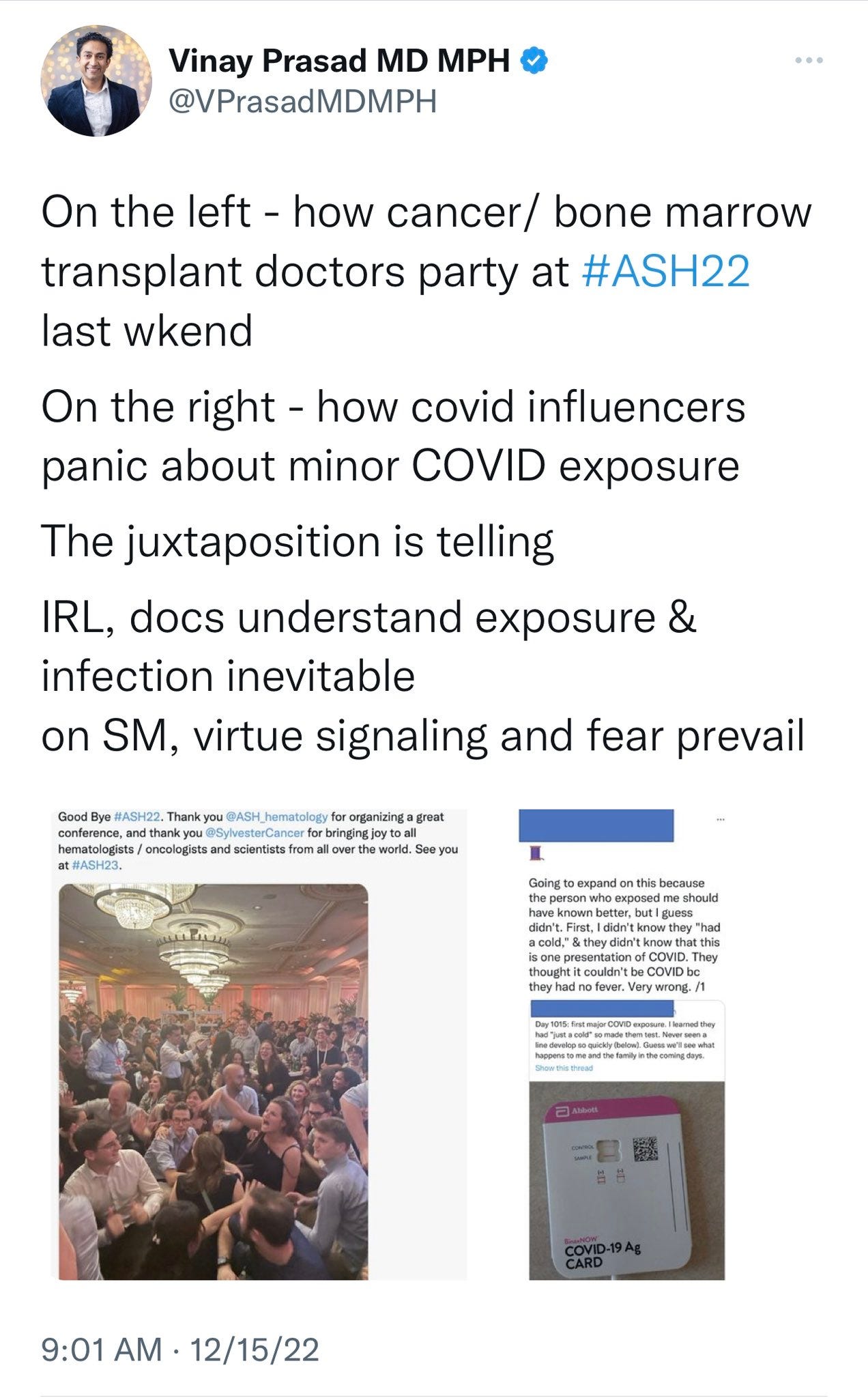
Over the past two years, there has been a string of in-person medical conferences with zero SARS-CoV-2 precautions in place - not even a PPE mandate. Many of these people would obviously become infected with a deadly & disabling virus there, and potentially be asymptomatic infectious. While the rest of the professional world may not care, the medical world has a specific obligation that requires extra precautions - as they work out of a hospital, seeing & treating patients who have all sorts of varying ailments, such as disabilities or having a compromised immune system.
In fact, many if not most of the people that need to go to a hospital have complications that put them as "high-risk" for having bad outcomes with a COVID-19 infection. With how contagious and dangerous SARS-CoV-2 can be to these people, who are still full human beings with dreams & desires, the hospitals that are supposed to treat their ailments *have* to take extra precautions to protect the health of their patients. As we've written before, the scientific fields of medicine and engineering must learn to work together to start beating back the SARS-CoV-2 pandemic, instead of entertaining so many rabid sealions that have wasted years boosting their own profile by concern trolling and misleading the public.

In turn, hospitals have stopped requiring masking, and have little to no precautions in place to prevent SARS-CoV-2 airborne viral transmission to patients. We've found numbers for deaths caused by hospital-acquired (nosocomial) COVID-19, and they’re horrific. One publication says it’s a 39.1% fatality rate, another publication says it’s a 57% fatality rate for “…patients with hematologic malignancy,” aka cancer, and another publication says crude mortality rate is around 10%. This is horrific. No professional standard would or should accept this level of failure.
Now you have doctors, nurses, and other HCWs partying unmasked at professional conferences, getting infected, and then bringing the virus to work and sabotaging the health of the people they've sworn a sacred oath to care for. How do you think this might feel to these patients? The disabled, the immunocompromised, and those who are now suffering from Long COVID? The shame of being unable to guarantee their health when they go to a hospital that they *must* visit, unlike the bars or indoor restaurants they currently have a choice to avoid.
In truth, there is also a great collective national shame, in that so many of us were organized to play a part in the killing and maiming of millions of our fellow Americans. Even worse, some are engaged in angry, violent denial that this even happened - screeching at frontline doctors who struggled to save lives in early 2020 that they were killing patients with ventilators, as the virus was somehow actually harmless. Across the political spectrum, we are now seeing wealthy white mostly-male professionals and academics scolding mostly-women - especially disabled, immunocompromised, and high-risk people who are forced to agitate for themselves and be their own activists, treating them as hysterical broads who need to leave it to the Public Health “experts."

The same experts who wasted years insisting that SARS-CoV-2 was not airborne, of course. Let’s not forget that little debacle! Here is virologist Joseph Osmundson in January 2021 making a soon disproven, outlandish claim:
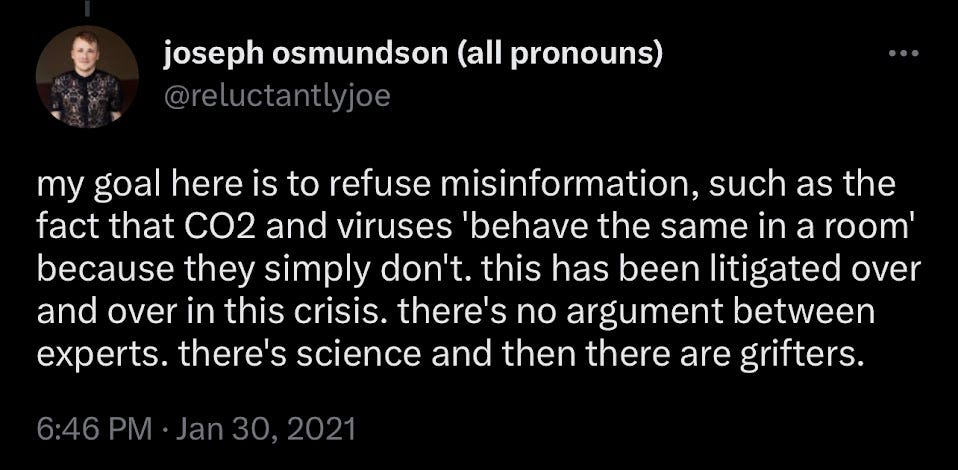
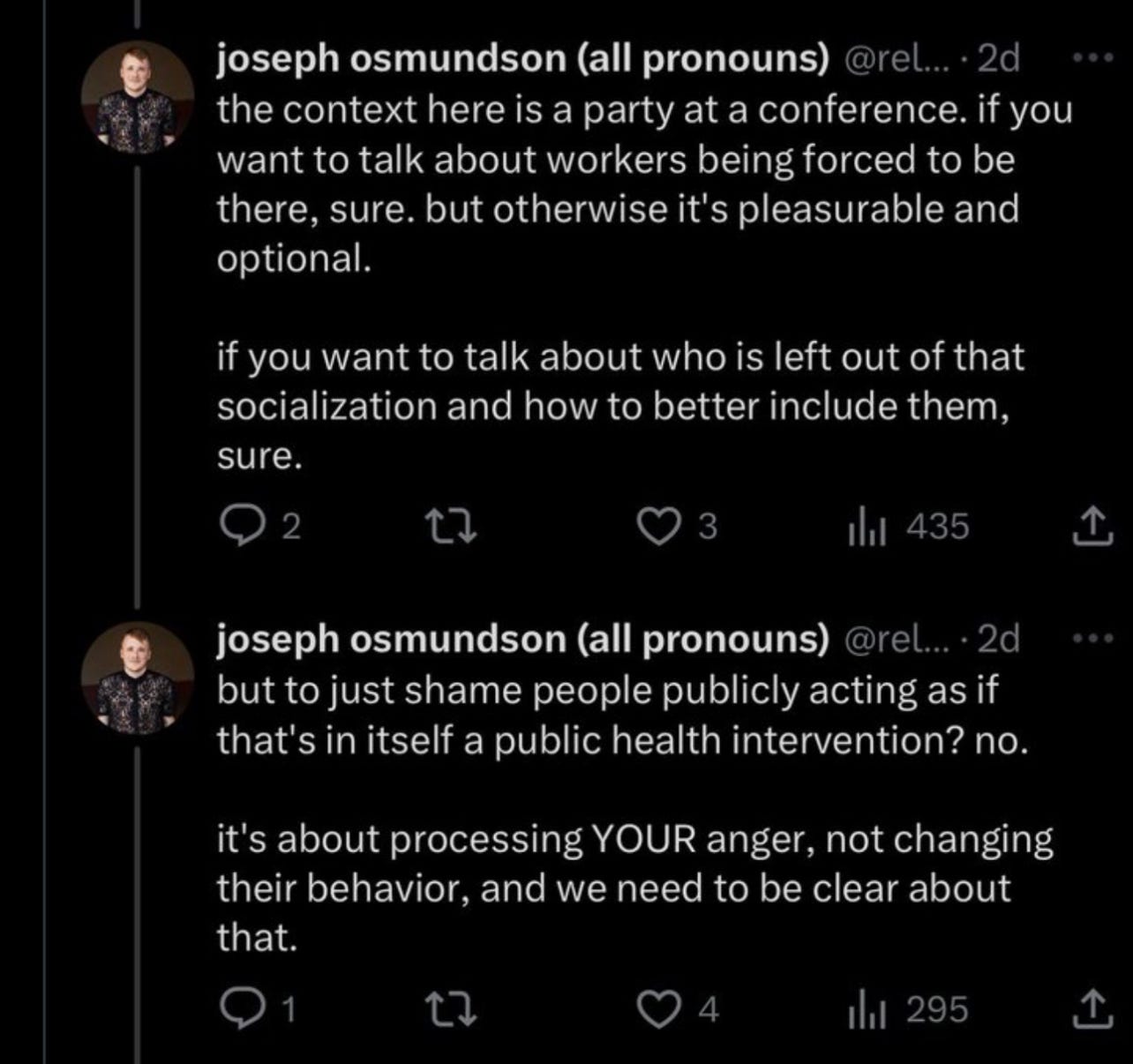
Anyone publicly making baseless accusations of grifting and being this gravely wrong needs to vastly reconsider how arrogantly they present themselves in public statements when talking about public health matters. Instead, Osmundson has simply doubled down on his childish behavior - we’ll come back to this.
Left to fend for themselves, the disabled, immunocompromised, and Long COVID communities have had to become their own activists and agitators, some taking to social media to raise hell about doctors and nurses risking SARS-CoV-2 partying at professional conferences, then bringing home the virus to the hospital where these patients are forced to visit in-person and risk exposure, forced to give up "normal" activities like bars, clubbing, parties, and other crowded in-person events where a deadly and disabling virus is allowed to freely transmit. You have to understand, these patients are forced to fight for themselves to protect their health from a still deadly & disabling virus - most also don't have medical degrees or the luxuries provided by an Ivy League education or a 6-figure STEM job.

It was originally eugenicist freakshow Martin Kuldorff of the Koch-funded Great Barrington Declaration who seeded the talking point that we must lie to ourselves and force people to live in denial of how SARS-CoV-2 & COVID-19 are socially transmitted through the air and can do countless harms to our bodies. Now, it has become mainstream liberal discourse, as championed by Ivy League academic Gavin Yamey, virologist Joe Osmundson, and the "Neoliberal Jon Snow" parody account, shouting down a group of mostly women, who are disabled, immunocompromised, or otherwise high risk for SARS-CoV-2 complications - and forced to become their own foot soldiers in a war to protect themselves from a virus that these well-off professionals are more than happy to freely infect themselves and others with.

As if these (mostly) women don't struggle with feelings of shame or frustration for being forced to live their lives in isolation, taking extra precautions, struggling to access the healthcare they need from hospitals that have let the SARS-CoV-2 virus spread. The "focused protection" that Martin's GBD and self-righteous liberals have refused to provide for these people never arrived.
Employ a little imagination and a splash of empathy, and you can start to try and feel the frustrations these people are feeling. Of course, both mass-infection advocates and enlightened COVID centrists agree - these people are hysterical and must be put in their place. Us well off professional duders just know better than you, and how dare you make us feel bad about all the fun we're having, putting your life and health at risk when you come to the hospital seeking essential care.
This is ridiculous behavior, full stop. There is no excuse for this. People are avoiding hospitals and the healthcare they require because they understand the extreme risks to their health aren't worth rolling the dice - whether it's an immunocompromised patient who can't risk a single SARS-CoV-2 infection, or a Long COVID patient who can't risk a reinfection worsening their symptoms. Instead of employing stricter prevention protocols to protect the lives of the patients they're sworn to protect, many doctors and professionals instead take to mocking these same patients, publicly and online.
This is childish, pitiful behavior, and should be disciplined with extreme prejudice. If you want the prestige and respect of a highly qualified professional, then you have to act like one as well - especially when you are publicly presenting yourself in a professional format. Some doctors, like Cardiologist Jonathan Reiner, have made it clear they take their professional obligations seriously, and that they support protecting patients from a deadly & disabling airborne virus. From the Annals of Internal Medicine that Reiner links to in the above tweet:
A compelling reason for continuing masking in health care is presenteeism, a behavior that long preceded, and will likely outlast, the pandemic. Health care personnel are notorious for coming to work while ill. In studies conducted during the pandemic, half to two thirds of health care personnel acknowledged working with symptoms of respiratory illness (5). Presenteeism has been well documented in health care–associated respiratory viral outbreaks (6), with various reasons proffered, including an unwillingness to place burdens on colleagues, a belief that some respiratory infections may be trivial, a fear of reprisal for absenteeism, a moral imperative to provide patient care, and, for those in some roles, a lack of paid sick leave. We can find no reason to believe these time-honored behaviors will change if masks come off.
On a macro scale, this disorderly breakdown between healthcare professionals and their patients is incredibly worrying. As a modern, civilized society, we rely upon central pillars to serve as the foundation for the liberties and luxuries we enjoy - and if hospitals are shifting into places that harm & humiliate patients, then we risk the beginning of a failure cascade that brings the rest of the whole damn charade down with us into a historic catastrophe.
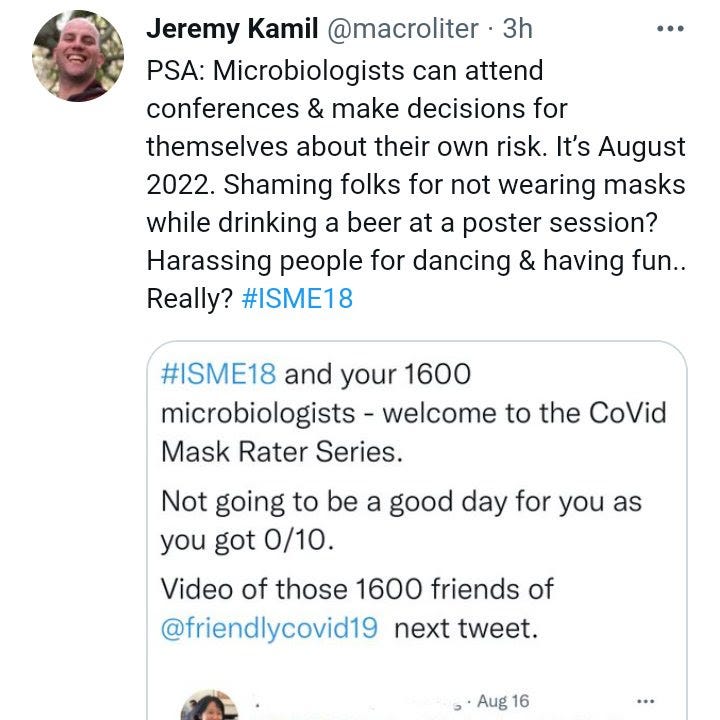
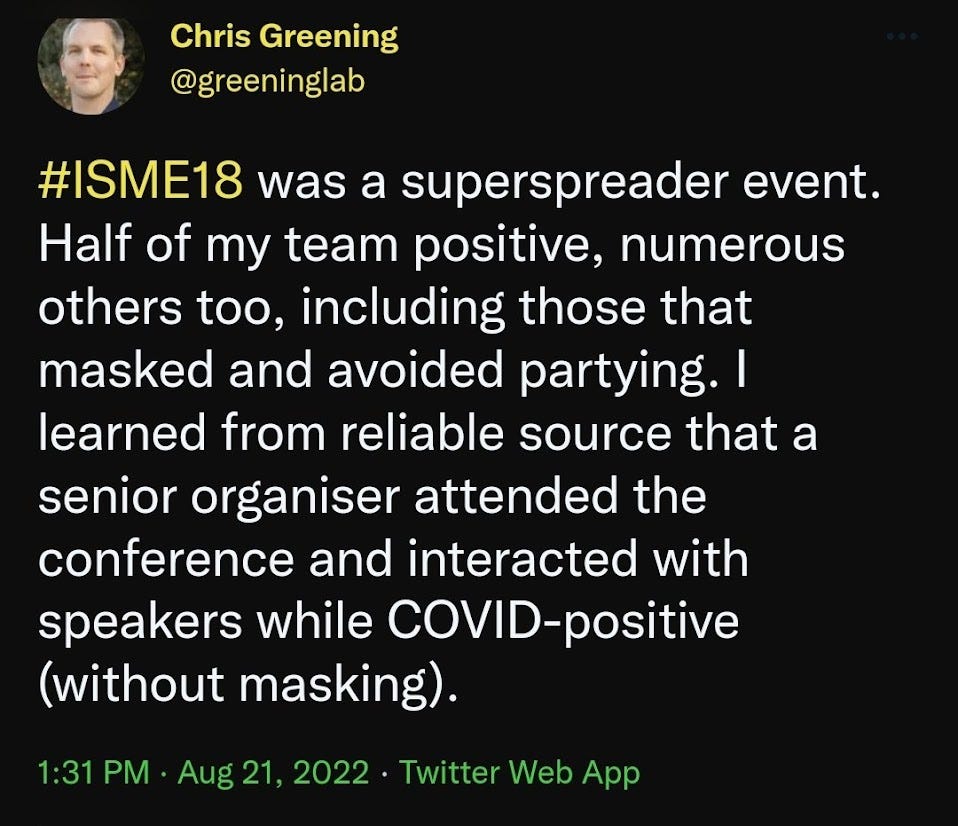
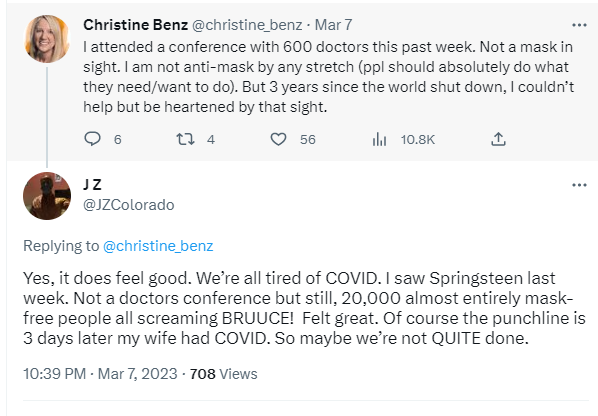
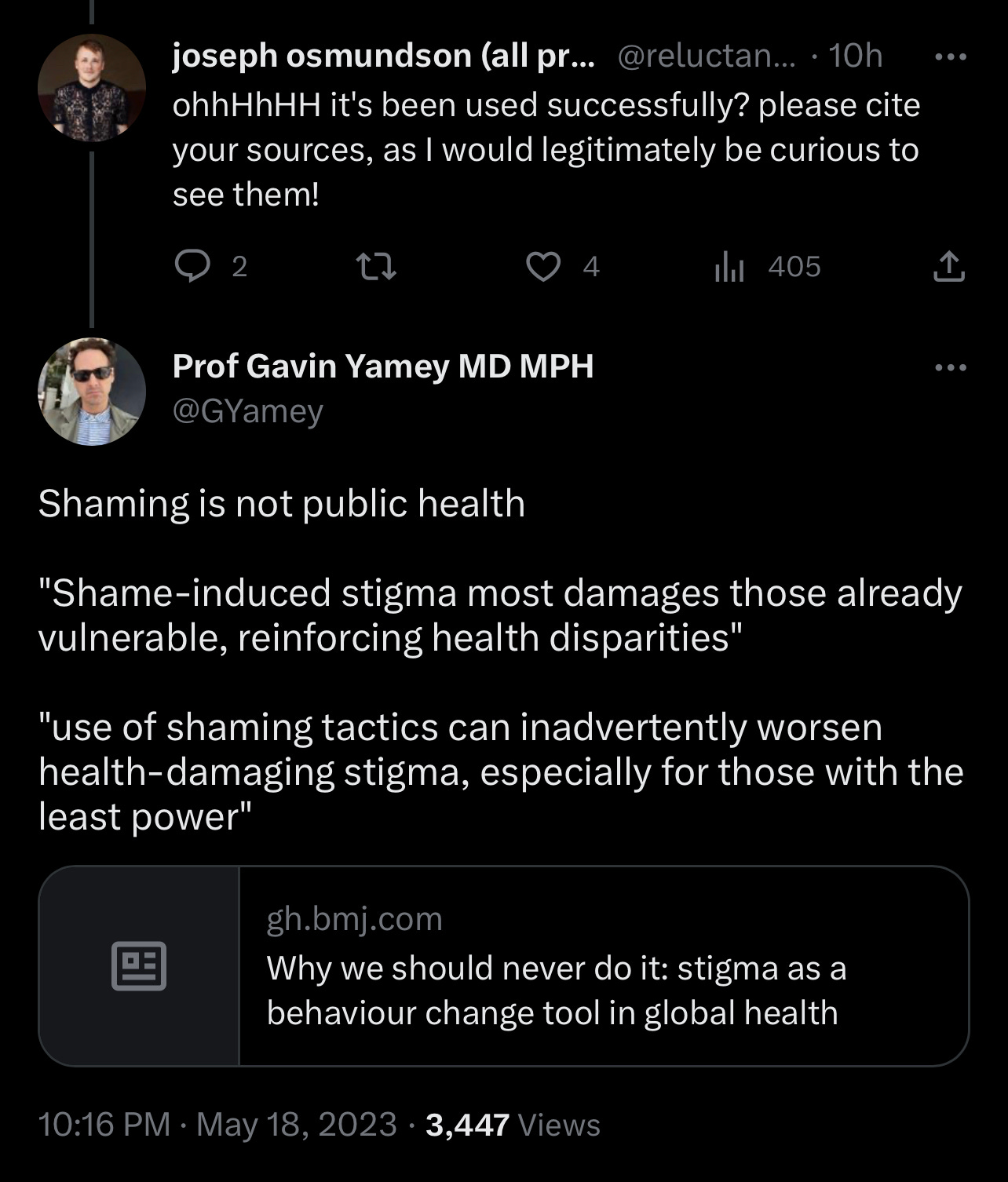
The whining about public criticism of unmasked medical conferences, award ceremonies, etc. - especially when the CDC just recorded a massive COVID-19 outbreak at one of their own conferences, with a 10% infection rate - is often from those that have "moved on" or have thrown any sort of precaution around SARS-CoV-2 out the window, willingly throwing their bodies at repeat infections with potentially lifelong complications that have already upended the lives of countless millions of Americans. The problem is that, especially when talking about healthcare professionals, is that after these conferences, these people go back to the hospital, potentially infectious, and spreading the virus to countless others, including fellow staff and most importantly, patients. Those trying to silence criticism by claiming that "shame" is ineffective public health, or making terrible comparisons to the HIV/AIDS epidemic, or themselves employing shame, are doing so because they themselves feel that very shame - and they don't want to.

These "professionals" want to write off the people who raised these concerns as unserious, childish, and not worth listening to. Doubling down on shameful behavior as a coping mechanism instead of acknowledging the harm that is being done, unsurprisingly. It's a matter of class politics, wrapped in ableism - the wealthy, able-bodied professionals who consider themselves "low-risk" that see themselves as simply on a higher social status, lording over the high-risk, disabled, immunocompromised, etc. as American healthcare is, by design, prohibitively expensive, as medical bankruptcies still dominate the American economic landscape.


As the Biden administration came into office in 2021 and immediately went to work dumping the entire burden of the pandemic onto the viral underclass, so went the sense of shared struggle & solidarity against a common foe. What you are seeing play out now is the endgame of this caste society project: the wealthy professional class with six figure salaries gets to party & ridicule the dirty cripples, the viral poors, the very people who have had to put their lives on hold to try and survive InfinityCOVID, as an airborne, socially transmitted virus still kills and cripples countless Americans weekly. Those who have had to become their own activists and agitators are forced to bear the burden that is supposed to be lifted by the very healthcare professionals who swore an Oath to protect & treat these patients.

Of *course* professionals like Yamey & Osmundson are whining about being shamed, because they know this entire charade is a shameful disgrace. However, they're too comfortable and well off in their academic and professional roles to take a stand in solidarity with these activists and lead by example, when they are frankly obligated to. Public health is a public effort, not to be decided in smokey backrooms by unhinged austerity fetishists, deli owners, & warmongering geriatrics. We all have to pitch in and help, especially when it comes to the most vulnerable in our society during an ongoing airborne pandemic.
If we are forcing high-risk groups like the immunocompromised, the disabled, those with Long COVID to fight for themselves, and engage in campaigns against the very people who are supposed to treat and protect them - then something is clearly very wrong, and we all need to make a change if we're going to get out of this crisis alive. Listening to childish, pitiful bullies who insult the most vulnerable and openly celebrate infecting them with a potentially fatal virus, at the damned hospital?
This will not end well for any of us.
Truth be told, we’ve known this fact since…1863, as written by the literal founder of modern nursing, Florence Nightengale, in Notes on Hospitals:
“It may seem a strange principle to enunciate as the very first requirement in a Hospital that it should do the sick no harm. It is quite necessary, nevertheless, to lay down such a principle, because the actual mortality in hospitals, especially in those of large crowded cities, is very much higher than any calculation founded on the mortality of the same class of disease among patients treated out of hospital would lead us to expect.”